Weight. Hair. Joints. Energy. It's often Vitamin D.
Vitamin D is a fat-soluble vitamin rarely found in food — primarily produced when UV-B rays hit the skin. Deficiency causes a cascade of problems: obesity risk, inflammatory joint disease, hair loss, and immune breakdown. Injections provide immediate, complete absorption that oral supplements can't match.

Vitamin D deficiency shows up in four distinct ways. All four respond to correction.
Most people think of Vitamin D as a bone vitamin. The real site covers four specific applications that go far beyond bone health — and all four are driven by a deficiency that affects 41% of US adults.
Low Vitamin D has been shown to be a cause of obesity. Studies comparing two groups — one supplementing Vitamin D, one not — found that the Vitamin D group lost weight faster. Vitamin D injections for weight loss support the metabolic processes that help the body shed fat more efficiently. Not a miracle cure, but a meaningful variable that is often overlooked in patients who struggle to lose weight despite consistent effort.
Vitamin D deficiency substantially increases the risk of inflammatory diseases, including rheumatoid arthritis. A 2018 study confirmed that people not getting enough of this essential nutrient are at significantly elevated risk for developing rheumatism. Complications from rheumatism can lead to osteoporosis in seniors. Vitamin D injections for knee pain and joint health correct the deficiency that is driving the inflammatory process.
There is a growing body of medical evidence linking hair loss to Vitamin D deficiency. Vitamin D is essential for stimulating hair follicles — without adequate levels, follicle function is impaired and hair loss follows. Alopecia areata, an autoimmune disorder causing patchy hair loss, has also been directly linked to Vitamin D deficiency. Injections correct the deficiency at the level that follicle stimulation requires.
Vitamin D is essential for calcium absorption and incorporation into bone. Without adequate Vitamin D, calcium supplementation is largely ineffective. Deficiency is a primary driver of osteopenia and osteoporosis — particularly in post-menopausal women on estrogen therapy. Injection provides the sustained elevated levels that oral supplementation often fails to achieve in patients with documented deficiency.
Vitamin D receptors are abundant in the brain — particularly in areas involved in mood regulation. Its deficiency is directly associated with depression, seasonal affective disorder, and chronic low energy. Correcting deficiency produces consistent improvements in energy and mood, particularly in patients who have been deficient for an extended period without knowing it.
Vitamin D is one of the most important immune regulators in the body — activating the innate immune response and preventing immune overreaction (autoimmunity). Deficiency directly impairs immune competence, increasing susceptibility to infections and inflammatory diseases. Injection achieves the sustained elevated levels needed for meaningful immune regulation.
Vitamin D deficiency is behind more symptoms than most patients realize — and it is easy to correct with the right delivery method.
Vitamin D is fat-soluble, which means oral absorption is variable and frequently inadequate for patients with documented deficiency. Injection bypasses this entirely. Costs are low — reasonably priced enough to pay out of pocket without insurance.
More than a vitamin. A hormone precursor.
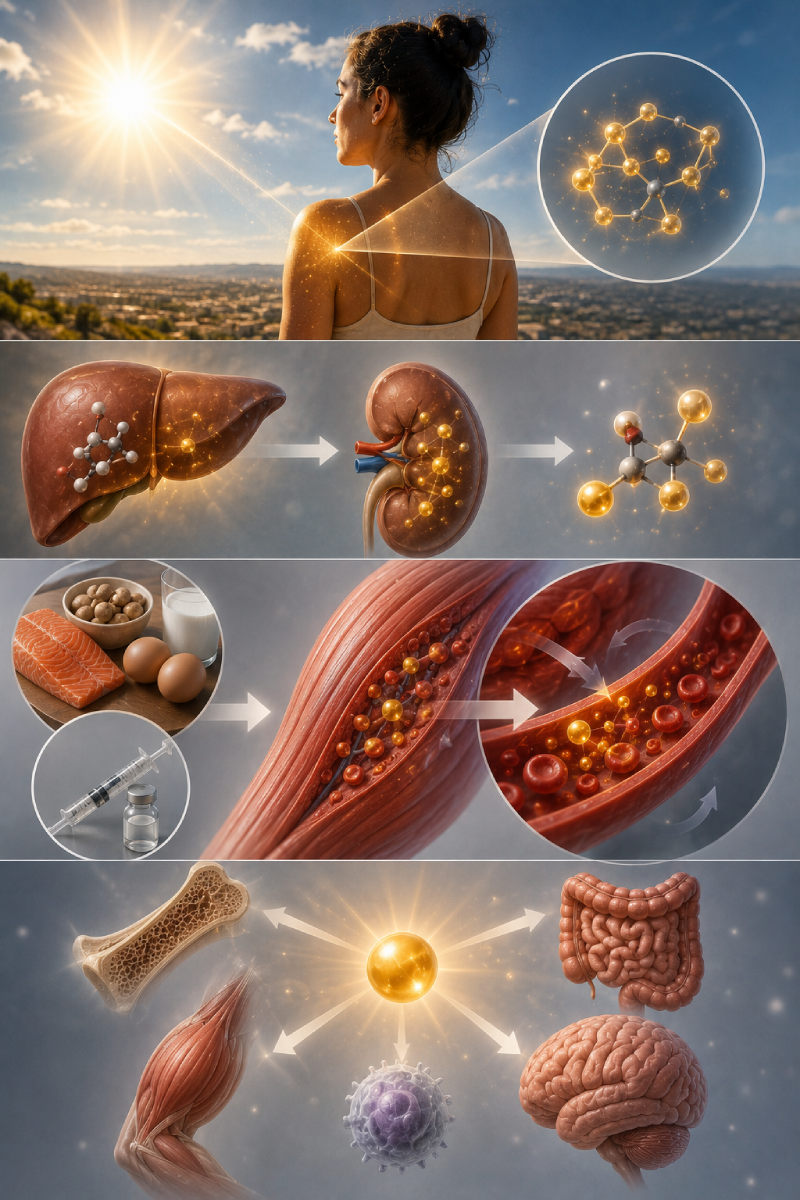
Vitamin D is a fat-soluble vitamin that is rarely found in the foods we eat. The primary natural source is UV-B radiation from sunlight — when ultraviolet B rays contact the skin, a reaction produces Vitamin D3 (cholecalciferol) in the body. In Las Vegas, despite abundant sun, many people are deficient because they work indoors, use sunscreen, or are in the sun during hours when UV-B intensity is insufficient. The vitamin then undergoes two hydroxylation steps — in the liver and kidneys — to produce the active hormone calcitriol, which binds to Vitamin D receptors in virtually every cell type.
Intramuscular injection deposits Vitamin D3 directly into muscle tissue, where it is gradually released into circulation over days to weeks — producing sustained elevated levels with a single injection. This is particularly important for patients with fat malabsorption conditions (Crohn's, celiac, gastric bypass) where oral fat-soluble vitamin absorption is unreliable. It is also the fastest route to correcting documented deficiency — achieving therapeutic levels far sooner than daily oral supplementation requires.
Serum 25-hydroxyvitamin D (25-OH-D) is the standard measure. Reference range: 30–100 ng/mL. Optimal therapeutic range for most clinical goals: 50–80 ng/mL. Below 20 ng/mL: clinically deficient — treatment is indicated. 20–30 ng/mL: insufficiency — treatment is appropriate for symptomatic patients. We measure 25-OH-D before prescribing and at follow-up to confirm correction.
The most common nutritional deficiency in America.
41% of US adults are Vitamin D deficient — and its effects span fatigue, immunity, mood, bone health, and hormonal function. Injection provides the most reliable correction for patients who don't respond to oral supplementation.
From deficient to optimally replete.
25-OH-D measured before any treatment. We confirm deficiency level and determine the appropriate loading dose vs. maintenance dose for your specific situation.
Intramuscular injection — typically into the deltoid or gluteal muscle. The fastest appointment in our clinic. Vitamin D3 is gradually released from muscle tissue over days to weeks, producing sustained elevated levels.
Retest 25-OH-D at 8–12 weeks to confirm correction. Maintenance injection monthly or quarterly depending on your baseline deficiency and sun exposure. Many patients maintain optimal levels with quarterly injections.
Medicine that
gets you.
We test before we treat and retest to confirm correction. Vitamin D dosing without monitoring is guesswork.
Always Test Before Treatment
We measure 25-OH-D before prescribing any Vitamin D protocol — deficiency, insufficiency, and adequate levels require different approaches. We don't prescribe loading doses without confirming deficiency first.
Follow-Up Testing Included
We retest at 8–12 weeks to confirm your levels have corrected to the optimal range. If they haven't — because of absorption, dose, or frequency issues — we adjust.
Injection for Non-Responders to Oral
For patients whose Vitamin D hasn't corrected with oral supplementation, injection bypasses the absorption variable entirely. Direct intramuscular delivery produces correction that oral supplementation in these patients cannot.
Integrated With BHRT Panel
Vitamin D is part of our comprehensive hormonal panel. Many patients discover deficiency when they come in for a BHRT consultation — and correcting it as part of their broader protocol often produces more comprehensive symptom relief than hormones alone.
Deficiency corrected.
Energy restored.
Everything you
want to know.
Vitamin D deficiency is
easy to fix. If you actually fix it.
A 25-OH-D blood test, a loading injection if needed, and a maintenance protocol to keep you in the optimal range. Free consultation.